36M with decreased appetite, nausea and loose stools
A 36 year old male patient farmer by occupation came to general medicine OPD with chief compliants of
Decreased appetite since 1 year.
Nausea and Vomiting since 6 months.
Loose stools since 6 months.
Tingling sensation in his both Upper Limbs and Lower Limbs since 10 days.
HOPI
Patient was apparently alright 1 year back then initially he had decreased appatite associated with nausea which was gradually progresed to complete loss of appatite with in 5-6 months but able to still manage his daily routine activities. Then patient developed vomitings, 4-5 episodes per day , greenish , immediately after food intake. With food particles as contents. Not a/w blood in vomiting.
Since 6 months patients had loose stools now increased in frequency since 2 months. 5-6 episodes per day, Watery consistency, large quantity, associated with greenish mucous with No blood in stools.
Then problem of passing loose stools has worsened in past 2 months.
There is a significant decrease in his body weight in past one year ( 70 kg --> 50 kg ).
Last month with similar complaints patient went to one of the corporate centers in nearest city and evaluated further where he also had intra hospital hypoglycemic attacks.
PAST HISTORY :
Not a known case of HTN , DM and TB.
FAMILY HISTORY :
No similar complaints in family.
PERSONAL HISTORY :
Appetite : decreased
Sleep : disturbed and inadequate
Diet : mixed
Bowel and bladder : irregular
GENERAL EXAMINATION :
Patient is concious, coherent and co-operative
Built : weak and malnourished.

There are no signs of dehydration.
Pallor : present

Clubbing : present

Cyanosis : absent
Lymphadenopathy : absent
Edema : bilateral pedal edema upto knees present(pitting edema)


Vitals :
BP : 80 / 60 mm Hg
PR : 110 bpm
RR : 20 cpm
Temperature : afebrile
SpO2 : 98 % (@ room air )
GRBS : 98 gm/ dl
SYSTEMIC EXAMINATION :
CVS : S1 & S2 Heard and no abnormal murmurs heard.
RS : BAE+ and NVBS.
ABDOMEN :
INSPECTION
Shape : mild distended
Umbilicus: normal
Movements : normal
Visible pulsations : absent
Skin or surface of the abdomen : normal
PERCUSSION- tympanic
AUSCULTATION : bowel sounds heard
CNS : no focal neurological deficits
INVESTIGATIONS
At his previous hospital
Hb : 9.6,
Albumin : 1 gm/dl,
Cytology:showed mixed inflammatory cells with negative malignant cells and lymphocytes
Chest X-ray : normal
USG abdomen : thickening of terminal ileal loop, moderate ascites, bilateral pleural effusion.
CECT Abd : Diffuse long segment circumferential wall enhancement of small bowel loops
Colonoscopy:non specific segmental colitis

MRI Abd : subcentrimetric lymphadenopathy and tiny rt renal cortical cyst.
H/o significant weight loss upto 20kgs with in 1 year.
H/o blood in stools present once a while .
At our facility
Hb : 8.3
Albumin : 2 gm/dl
USG abdomen : Submucosal edema of multiple small and small bowel loops with moderate ascitis.
Short segment intussusception in large bowel at left hypochondrium.
ECG :


ABG :
pH 7.57
pCO2 : 19.8
PO2 : 114
Hco3 : 18.5
St. Hco3 : 22.8
Spo2 : 98
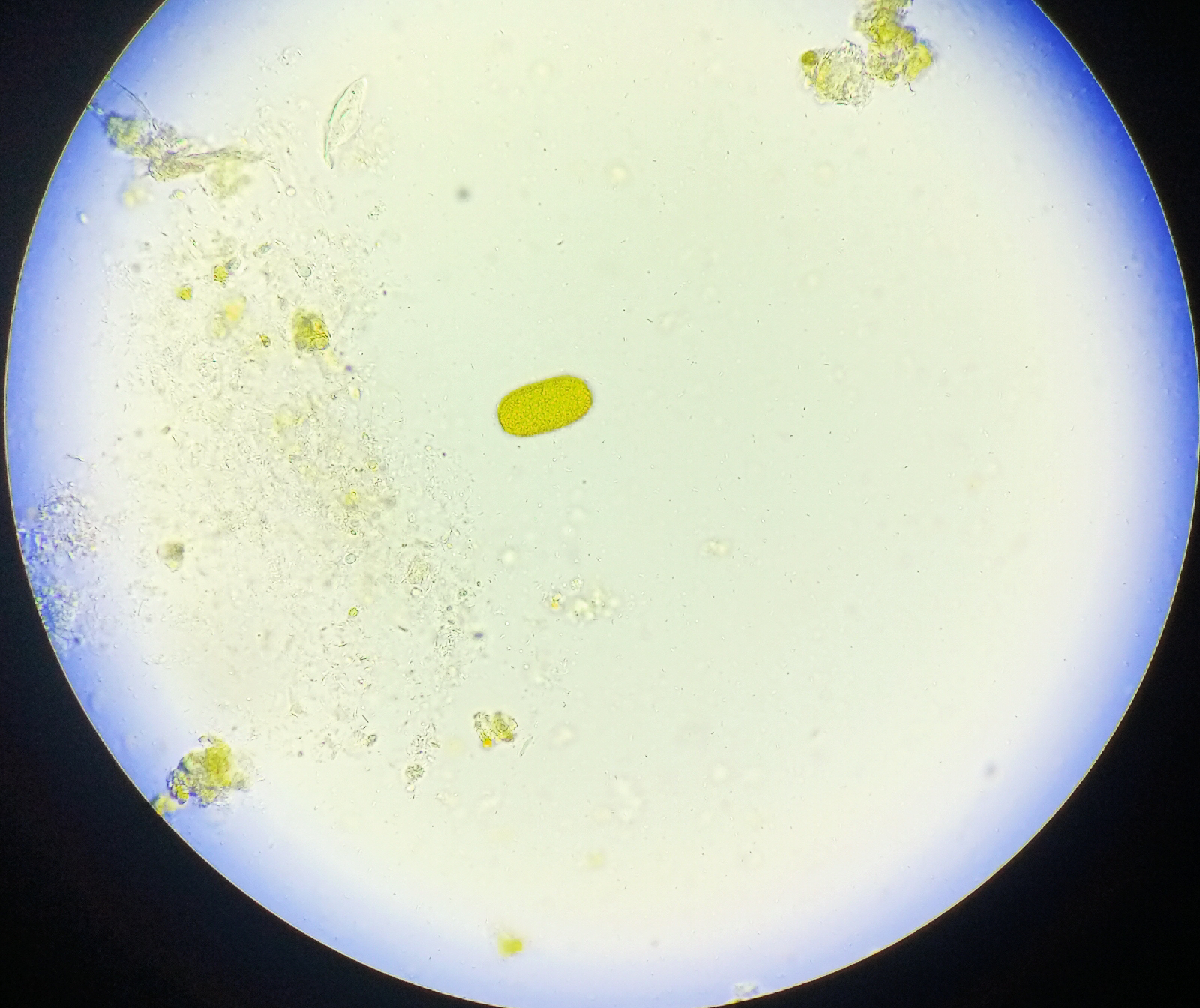
Stool microscopy reveals eggs of Capillaria Philippinesis.

Provisional Diagnosis : Chronic diarrhoea under evaluation.
D/D :
Inflammatory bowel disease
Protien losing enteropathy
Whipples disease
Malignancy
Treatment:
Iv fluids 1 unit NS @ 75ML/HR
T.Albendazole 400mg
Inj. Zofer 4 mg sos
Inj. PAN 40 mg IV BD
Inj. Optineuron 1 amp in 100ml NS IV OD
Inj. PCM 1 gm IV sos if Temp >102F
Tab. Loperamide 4mg po BD
Tab. Sporolac DS po TID
Ors sachets 1 packet in 1 ltr water.
HIGH Protein Deit.
GRBS 4th hourly.

Stool microscopy reveals eggs of Capillaria Philippinesis.




Comments
Post a Comment